For more than two decades, the dominant explanation in health policy research has been simple: it is the prices. Early last year, however, some commentators began arguing that spending growth was being driven primarily by utilization and service intensity, not prices. So what’s the right answer?
The United States spends roughly $5.3 trillion annually on health care — 18% of GDP and far more per capita than any other wealthy nation. The U.S. pays more for the same drugs, procedures, and physician visits than virtually every comparable country due to opaque price-setting; the absence of government-administered fee schedules or reference pricing for private payers; weak insurer bargaining power against consolidated health systems; and a lack of price transparency that allowed enormous variation between payers for identical services.
Earlier this year, however, an article in Health Affairs suggested that it’s not high prices but high utilization that is driving high health care spending, particularly expensive products like the GLP-1 drugs used to treat diabetes and obesity.
So, which is it? High prices? Or high utilization?
Last month, a trio of economists re-examined the question and discovered that increases in utilization are often actually just price increases in disguise.
Particularly when there is no clear evidence that patients are sicker or receiving meaningfully different care, it very well can be that changes in intensity reflect an impact on prices, not volume.
Another similar example is for the administrative costs faced by providers in relation to billing. While the NHE estimates do account separately for the administrative spending incurred by payers and insurance, they are not able to do the same for provider-facing administrative costs, such as billing, coding, and prior authorization compliance; instead, these administrative costs are embedded in estimates of provider spending. Several studies have nevertheless shown that these costs are large, growing, and significantly greater than in other countries. These costs, like upcoding, ultimately raise the price we pay for care without increasing the volume of care delivered.
If price indices for health do not correctly capture a substitution effect (e.g., upcoding) and administrative costs faced by providers, they are likely to overestimate intensity.
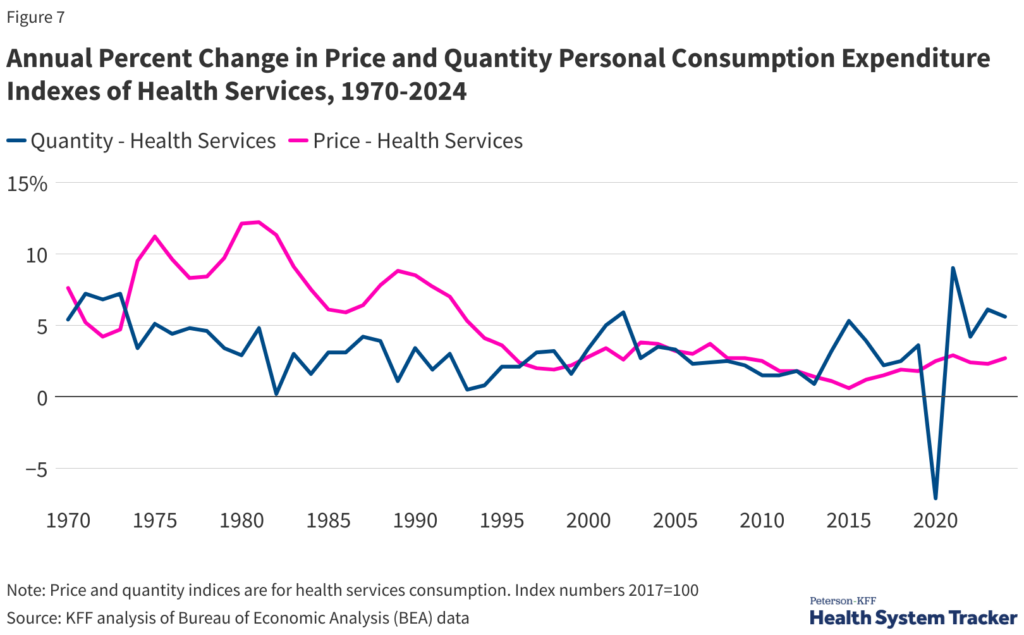
That’s not to say that utilization has not increased. Data from the KFF indicates a noticeable increase in health care usage following the COVID pandemic.
But two things can be true at the same time — Americans can be using more health care and health care prices can be increasing at an unsustainable rate. In fact, there is some evidence that health care expenditures may actually be undercounted.
So, what’s the solution?
The solution to America’s health care affordability crisis is not to tell people not to go to the doctor. Americans are already skipping health care due to concerns about affordability. Instead, we need to improve the value of health care by providing patients and employers who pay for health care with accurate, transparent information about prices and quality so they are empowered to make informed choices when shopping for their health care needs.